This past month I attended the National Farmworker Health Conference in Denver, Colorado. This year’s conference marked the 50th anniversary of the passage of the Migrant Health Act and honored the historic first comprehensive efforts to provide health services to the migrant farm worker population in the U.S. As someone who is new to the community health center movement, I came to the conference with only a basic knowledge of the Migrant Health Program. It was a privilege to hear leaders, advocates and clinicians in the migrant health community speak about their struggle and commitment to better the lives of farm workers in this country. I was particularly moved to hear Dolores Huerta, co-founder of United Farm Workers of America (UFW), present the keynote speech. She spoke about her role in the UFW’s struggle to organize and the many connections and parallels between their fight and the mission and work of the migrant and farmworker health program.
Passed in 1962, under the John F. Kennedy administration, the Migrant Health Act initiated the first federally-funded primary care program in the U.S. and was a precursor to the authorization of the consolidated community health center program. The Migrant Health Program aimed to address the disparities in health care access experienced by the migrant and seasonal farm worker population. Historically those who grow and harvest our crops have been the poorest and most recent arrivals to this country and consequently the most disadvantaged, vulnerable and exploited. Migrant farm workers were excluded from the National Labor Relations Act and thus disallowed from good-faith collective bargaining with their employers. Their wages have remained low, their work has been unstable and they have typically been a difficult population to organize. The United Farm Workers, which began with the merger of two farmworker’s rights organizations, and whose origin coincided with the launch of the first neighborhood health centers in 1965-1966, waged the first successful campaign to unionize farm workers. Their campaign used a non-traditional community organizing model that focused on small and localized outreach. Led by Cesar Chavez and Dolores Huerta, the UFW met with workers face-to-face in the fields and held house meetings where they talked with the laborers about their working conditions and educated them about their collective power. Through these efforts, they gradually gained the support and trust of workers and initiated a grassroots movement to organize and unionize.
The migrant health model has also employed non-traditional strategies to ensure that migrant and seasonal farmworkers have access to primary and preventive health care services. Today, 159 migrant health centers serve nearly 900,000 farmworkers annually.
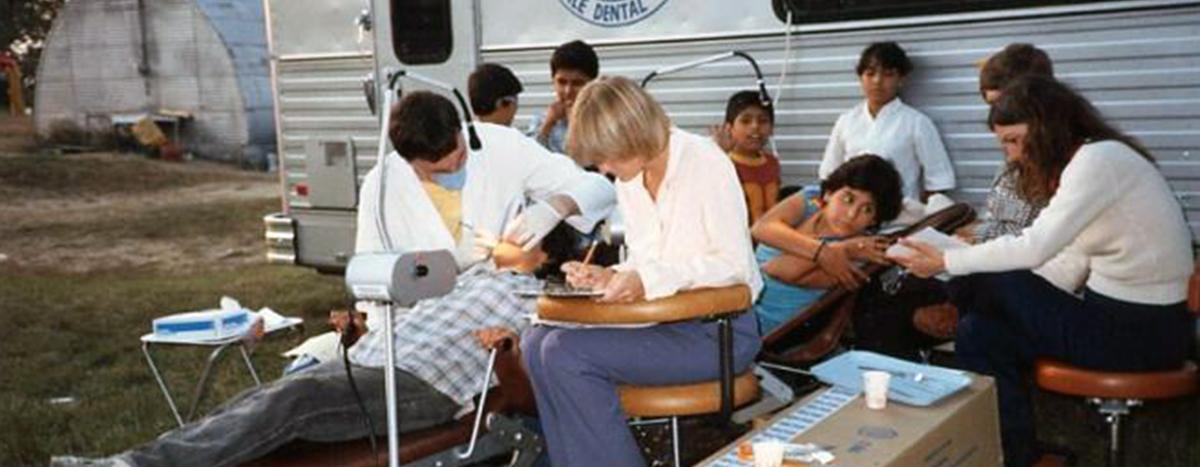
At the conference I heard from outreach workers who travel every day - sometimes as far as 50 miles in mobile health vans - to provide primary healthcare services to workers laboring in the fields, often spending full days under the hot sun in difficult conditions. Some migrant health programs have collaborated with growers and advocates to improve housing conditions for the migrant population and their families who previously lived in unsafe and unsanitary work camps. Another important aspect of migrant health programs is patient education about nutrition, infectious diseases, pesticides and work-related injuries. In order to be effective, the migrant health centers have had to respond to the unique challenges of treating the migrant farm worker population, which include language and cultural barriers, unstable and transient working conditions, and fear and isolation due to immigration status.
The migrant health program, and the health center movement as a whole, has deep roots in grassroots social struggles and has been shaped by this history. In listening to speakers on the various panels and in group discussions voice their challenges and goals for the future, I realized how intertwined the migrant health program’s mission is with other social justice issues. Migrant healthcare providers have a clear understanding about how exploitative labor laws, unhealthy working conditions, draconian immigration laws and other forms of oppression and inequity have impacted their patients’ health. They, and other community healthcare providers, have an obvious imperative to advocate for universal access. As advocates and providers of care for the traditionally underserved we should also be committed to the fight for workers rights, comprehensive immigration reform and environmental justice in order to truly defend and protect the health and well- being of the communities we serve.
By Nicole Rodriguez-Robbins







